

What is it?
Common Conditions
Common conditions that affect the elbow are:
- Painful stiff elbow
- Pain on outside of the elbow on use
- Pain on the inside of the elbow on use
- Swelling on the back of the elbow
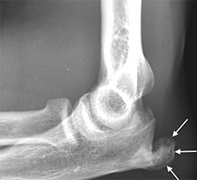
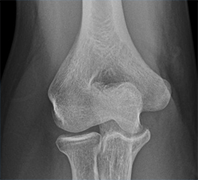
Symptomatology – A Painful Stiff Elbow – Typically a painful stiff elbow may be an indication of underlying arthritis or previous injury to the elbow at a younger age. Simple x-rays will confirm any evidence of arthritis in the joint. CT scan can also be requested which will give more information on the degree of arthritis and bone quality.
Younger patients with arthritis in an elbow from a previous injury can benefit from physiotherapy and anti-inflammatories.
If your imaging is suggestive of a loose body in the elbow (small calcified areas of bone around the joint) and if these are giving symptoms of pain and locking then surgery in the form of open debridement may be advised. The elbow is approached from the back through a small incision, the loose body is removed and any arthritic bone is debrided. This can have very good results for pain relief and can lead to a modest improvement in range of movement. Elbow replacement in younger patients is not indicated as the longevity of elbow replacements in a demanding younger patient is not satisfactory as a good treatment for the patient.
Elbow replacement is often the last resort in an arthritic elbow which is painful and stiff and this is reserved for older patients usually above the age of 65 to 70. Surgery involves general anaesthetic, the elbow is approached from the back through a long incision, the arthritic bone is removed and metal implants are cemented to both the upper arm bone (humerus) and the ulna. Patients normally go home within one to two days and the same risks apply as for any joint replacement of infection, bleeding, nerve injury, fracture and stiffness. Results are good for pain relief and there may be improvement to a certain extent in range of movement.
Symptomatology – Pain on the outside of the elbow
Pain on the outside of the elbow can represent a condition referred to as tennis elbow, also known as lateral epicondylitis. Typically there is no history of an injury but a chronic dull ache is felt over the outside of the elbow. This is worse on lifting things, for example lifting a suitcase into the boot of the car, pouring a kettle and opening jars. The tendons at the bottom of the upper arm bone attach across the wrist, so extending your wrist may precipitate pain on the outside of the elbow. If you present with these symptoms, I would need to exclude any underlying arthritis on that side of the elbow. If arthritis is excluded then treatment for tennis elbow can include physiotherapy, electrode therapy, ultrasound therapy, massage, anti-inflammatories, tension strap. In my own practice I do carry out steroid injections done in a Barbitage technique on the outside of the elbow. Current evidence is that this does not cure the condition but can reduce symptoms to a tolerate level until it self resolves. Other injection treatment is available but studies have shown no improved benefit long term than a simple steroid injection. Tennis elbow is a self-resolving condition which can go on for 12 to 18 months. In resistant severe cases of tennis elbow, surgery may be considered particularly if a patient has tried all conservative measures and has had symptoms for over a year then an operation may be advised. This is done under a general anaesthetic, approximately a two inch incision is made over the outside of the elbow, the tendon that is inflamed is released from the edge of the bone, the bone is divided, the tendon decompressed and then the wound closed. The arm is then rested in a bandage and sling for two weeks. Physiotherapy is then required thereafter. The overall success rate is 85% and recovery is a minimum of three months.

Symptomatology – Pain on the inside of the elbow
Pain on the inside of the elbow can often be from what is referred to as Golfer’s elbow, also known as medial epicondylitis. If the pain is simply over the bone prominence, worse on flexing the wrist and in Golfer’s terms, it is the follow through that exacerbates the pain. In a right handed player it will be on the inside of the right elbow. Treatment and natural history of this condition are almost identical to a tennis elbow condition and surgery in the form of release and debridement is reserved for patients who have failed all conservative treatment and have severe enough symptoms after 12 months.
If the pain on the inside of the elbow is associated with electrical shock symptoms which go down the arm into the little finger and paraesthesia (altered sensation) then I will need to consider whether the pain is arising from the ulnar nerve and you can see more information on this condition under nerve entrapments of the elbow and hand.

Symptomatology – Pins and needles in my hand – peripheral nerve entrapment
Cubital tunnel Syndrome or Ulnar Nerve Compression at the elbow – the ulnar nerve runs around the back of the elbow. It is quite common to have symptoms from the nerve if it is being compressed around the back of the elbow. This manifests itself as pins and needles and tingling in the little finger and half of the ring finger. There can be an associated aching on the inside of the forearm. It is often worse when the elbow is flexed, typically it may wake the patient up from sleep at night because most individuals tend to sleep with the elbows bent. It can come on when reading or when on the phone. If it progresses this can manifest as subtle weakness in the hand, this can cause difficulties with fine movements and if it progresses the little finger may be seen to drift from the other fingers in an outward manner.
If symptoms are fairly mild and really limited to occasional night symptoms, then no intervention is required. If symptoms are becoming frequent and affect daily life then surgery may need to be considered. If there is persistent nerve deficit such as persistent numbness or weakness in the hand, then surgery would be needed.
With ulnar nerve entrapment it is essential to have an x-ray of your elbow and some nerve conduction studies. The nerve conduction studies will assess how the nerve is functioning as it crosses your elbow. If your nerve studies are normal this does not mean you do not have cubital tunnel syndrome / ulnar nerve entrapment. The nerve tests are supportive and helpful diagnostically to a certain extent but do have their limitations.
Surgery for ulnar nerve entrapment involves a small incision at the back of the elbow, the nerve is released as it runs through a little tunnel at the back. Surgery takes approximately 45 minutes, it is carried out under a general anaesthetic and you may be able to go home the same day. The elbow is rested in bandages and a sling for a few days.
If there are signs of significant weakness in the hand or if there is evidence that when you bend your elbow the nerve is subluxing (snapping out of position) then it may be essential to not only decompress the nerve (release) but to transpose it (move it from its position behind the elbow to the front of the elbow). This takes slightly longer and does carry a slightly higher risk of damage to the nerve. The nerve is brought to the front of the elbow and buried either beneath the muscle or under the skin. If this is carried out I ask that patients rest the elbow for a couple of weeks in a sling in order for the nerve to bed into its new position.
If the condition is diagnosed early then the outcome of surgery is excellent. The paraesthesia should resolve, fairly quickly. Improvement can take anywhere between six and twelve months. If you already have muscle wasting in the hand and weakness then often this will not recover however.